
Aquatic Injuries
by Gerald M. Dworkin
Printed in May 1986 jems


Each year approximately 10,000 new spinal cord injuries are identified and treated in this country. The average age of onset is 28.7 years with the most common age being 19 years. Fifty percent of the injuries occur in the 15-24 age group. Eighty-two percent of all spinal cord injuries happen to males.
The following statistics represent the etiologic causes of spinal cord injury in this country: A) motor vehicles 36.5 percent; B) falls 15.8 percent; C) gunshot U.6 percent; D) diving 10.6 percent; E)others 24.5 percent.
Cause and Effect
The major cause of these devastating traumatic injuries is, as would be expected, motor vehicle accidents. However, sports and recreational activities rank second as a cause of spinal cord injuries, and within this category, water-related activities are most numerous. Sports or recreational activities that take place in the water and which create the potential for spinal injuries include: wind surfing, bodysurfing, board surfing, water skiing, power boat and jet ski/bike recreation and competition. EMS personnel need to be prepared to handle this type of emergency with both knowledge and skills, as well as the appropriate equipment.
The Consumer Product Safety Commission (CPSC} estimates that each year, there are approximately 13,000 diving-board related injuries serious enough to be brought to hospital emergency rooms and 800 spinal cord injuries caused by diving accidents. According to the CPSC, ” . . . one of the major accident patterns associated with swimming pools was striking the bottom or sides of the pool because of insufficient depth for diving or sliding,” and further that “in addition to striking the bottom of the pool, people are injured when they hit protruding waterpipes, ladders or other objects in the pool.”
Diving should be strictly prohibited in shallow water. Over half of the pools in the U.S. are above-ground vinyl swimming pools, most of which have a constant depth of three to 3-1/2 feet. In order to gain entrance into a pool of this type, a ladder or platform is normally provided. Many injuries occur each year when children or adults attempt to dive into the pool from such structures.
The mechanism of injury is dependent on the fact that the victim is propelled head first which makes contact with some part of the pool. The position of the head and neck, the impact site, and the direction of the cervical spine determine the resulting cervical fracture. As a result of the impact, the head and neck are either flexed, neutral, extended, laterally flexed, or rotated, and the cervical spine is subjected to bending, compression, tension, shear, or torque.
Any victim of a diving accident should be suspected of having a spinal cord injury and handled accordingly.
Preventing Aquatic Spinal Injuries
Emergency services personnel can play an integral role in educating the public on the prevention and handling of spinal cord injuries in the aquatics environment.
The National Swimming Pool Foundation (NSPF), in cooperation with the National Spa and Pool Institute (NSPI), produced an eight minute film, “Learning How to Dive,” on safe-diving techniques. The use of this film is an ideal way to instill the importance of proper diving techniques and can be used in a school classroom setting, or at social, recreational, or educational gatherings of youth groups. The film can also be integrated into organized progressive swimming courses conducted through the American Red Cross, the YMCA, and the Boy Scouts of America.
“Learning How to Dive” tells the story of a young boy who broke his neck when diving into shallow water. The film provides instruction in proper diving techniques with the help of 1984 Olympic Gold Medal Diving Champion, Greg Louganis, U.S.Olympic Coach Ron O’Brien, and actor Patrick Wayne. EMS personnel can promote the use of this film within school systems, summer camps, community and private aquatic programs, etc.
EMS personnel can also work closely with their local aquatic facilities to ensure that the facilities are adequately equipped with appropriate rescue equipment (i.e., spinal immobilization devices and adjunctive spinal immobilization equipment). Their efforts can be coordinated with those of the local lifeguard services to assist them in their emergency response and emergency communication systems, and they can promote the need for trained lifeguards certified in CPR basic life support. Emergency service personnel can even provide additional training to the lifeguards in the area of oxygen administration and advise the facility management on the purchase of emergency equipment which would be compatible with their own. Emergency service personnel can also provide guidance in the development of plans for rescue and evacuation procedures during fire, chemical and chlorine gas emergencies.
Treatment of Spinal Cord Injuries
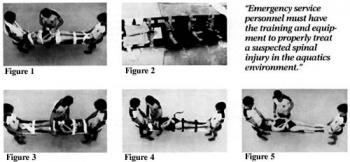
There are a variety of effective spinal immobilization devices (SID)for water rescue. The following figures demonstrate the use of the following SIDs:
- traditional wooden backboard (figure 1);
- ABS plastic backboard [Associated Medical Devices – figure 2);
- portaboard™ [Packaging Corporation of America – figure 3);
- aluminum spineboard (Ferno Washington – figure 4);
- scoop stretcher (Ferno Washington – figure 5);
It has been found that the pictured ABS plastic backboard and the Portaboard provided the greatest support and protection to the victim in the water due to the design of the particular SID and the lateral protection afforded the victim from wave action and water movement.
Handling Victims in Shallow Water
If the victim is found in a prone (face down) position in the water, the victim must be carefully rotated to a supine (face up) position. To do this, the rescuer must be careful to avoid any bending or twisting of the patient’s neck and torso to prevent any aggravation of existing injuries.
The rescuer places one forearm along the length of the victim’s sternum with the hand of that arm supporting the bony structure of the victim’s lower jaw. The rescuer’s other forearm is simultaneously placed along the length of the victim’s spine with the hand of this arm supporting the victim’s head at the base of the skull. The rescuer then supports the victim’s head and torso with the forearms and hands with an inward and upward pressure. The rescuer submerges, while maintaining this support position on the victim, and rotates the victim to a supine position [figures 6 & 7).
Once the victim is in a supine position, the rescuer then continues to support the victim from the side by placing one hand behind the neck and the other hand along the victim’s back. This technique will maintain proper alignment of the victim and will keep him in a horizontal and supine position. Additional rescuers should bring the necessary equipment (i.e. backboard, straps, lateral head/neck restraint, etc.), and a cervical collar should be positioned around the victim’s neck (figure 8).
To place a spinal immobilization device under the victim, rescuers should position themselves at each end of the device, which is floated alongside the victim in the water. On command, the rescuers lower the SID beneath the victim and allow it to come up slowly until he is completely supported. Care must be taken during the ascent of the device to properly align it with the victim. The first rescuer is responsible for maintaining the victim in alignment, in a supine position, until this is accomplished. Once the device is in place and the victim is adequately resting on it, the first rescuer may then begin immobilizing the victim to the SID [figure 9).
Sandbags, or other suitable head and neck lateral immobilization restraints, are placed along both sides of the victim’s head in order to reduce the risk of any lateral movement. Once this is accomplished,the immobilization of the victim to the SID may begin.
The following sequence is recommended for securing the victim to the spinal immobilization device using traditional straps or cravat bandages (figure 10):
- Across the chest.
- Above the waist to include the arms at the sides.
- At the hips to include the hands at the sides.
- Above the knees.
- Below the knees.
- Across the forehead.
- Other – to include feet or other areas for additional support.
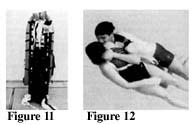
This technique of immobilization allows for the greatest mass of the body to be secured prior to securing the head. This reduces the risk of aggravating injury to the cervical spine should the body move due to wave action [figure 11).
Treating Victims in Deep Water
Victims with suspected spinal injuries in deep water should be turned from a prone to a supine position and then floated to shallow water, where they can then be immobilized onto an appropriate SID. However, in aquatic facilities which have a uniform deep water area (i.e., diving wells) or those facilities where the deep water is divided from the shallow water by a buoyed line, bulkhead, or other obstruction, the SID must be brought to the victim. First, flotation collars or other suitable flotation devices should be attached to their spinal immobilization devices. The flotation device is placed on the upper half of the SID only, in order to allow the rescuers to submerge the lower half under the victim [figure 12).
The flotation device should be kept attached to the SID at all times. However, the flotation device must allow for easy removal while the victim is immobilized to the SID for ease in transportation by ambulance to the medical facility
The victim in deep water is rotated from the prone to the supine position in a similar manner to the technique used in shallow water. This same technique can also be used for the victim who is submerged and who may be lying on the bottom of the pool or open water facility. However, the rescuer must use extreme caution when recovering the victim in order to assure that the victim is maintained in an aligned position while being brought to the surface. To do this, the rescuer supports the victim, as previously described, and swims diagonally to the surface while rotating the victim to a supine position.
The placement of the flotation SID under a victim in deep water requires two to three rescuers. It is preferable that the rescuers wear some type of personal flotation device (PFD), Mae West, buoyancy compensator, or a rescue buoy
Rescuer #1 rotates the patient to, or maintains the patient in, a horizontal position. Rescuer #2 places a cervical collar around the victim’s neck while Rescuer #3 positions the flotation SID in preparation for placement under the victim. The foot end of the flotation SID is placed at the victim’s head. Rescuer #1 supports the victim’s head/neck with one hand and guides the flotation SID with the other in order to prevent the SID from hitting the victim. Rescuer #2 and #3 grab the victim’s upper arm in close proximity to the armpit, and slide the victim up the flotation SID. Because the lower half of the flotation SID has no flotation attached, it can be easily submerged for this purpose. The support provided by the water, and the flotation SID, provides sufficient support for the entire body {figure 13).
Once the victim has been placed appropriately onto the flotation SID, the head is temporarily immobilized by the use of a lateral restraint device (i.e. sandbags) and the straps secured properly for immobilization of the torso, extremities, and head.
Once secured, the victim should be floated along the long axis of the body to the platform (dock, pool, side, shore, boat, etc.) for removal from the water. The head of the flotation SID can be pulled onto the platform while the foot of the device is allowed to drop deeper into the water.
To expedite the handling of suspected spinal injuries in open water areas where additional protection of the victim may be required, the flotation basket stretcher can be used. This device consists of a standard basket stretcher with a suitable SID secured within it, and a flotation collar attached around the upper half of the stretcher. The SID should only be secured at the head and foot of the basket stretcher so that it can easily be removed. The patient immobilization straps are attached to the SID and not to the basket stretcher.
This flotation basket stretcher is especially beneficial in white water rescue operations and when the victim is being handled in surf, moving water or cases when the victim will be transferred from the water to a boat. Marine vessels (police, fire, Coast Guard and lifeguard boats) and guarded surf beaches would greatly benefit in their patient handling abilities by using this device.
The placement of the flotation basket stretcher under the victim and the immobilization of the victim into the device are very similar to the techniques used to immobilize the victim onto the flotation spinal immobilization device.
However, after removal of the flotation basket stretcher from the water, the two straps securing the head and foot of the SID to the basket stretcher are removed. This allows the SID, with the victim attached to it, to be removed from the basket stretcher for patient transport to the medical facility Figure (14).
Summary
To reduce or eliminate spinal injuries in the aquatic environment, general principles for safe behavior must be practiced and enforced. Facilities responsible for providing aquatic recreational opportunities must implement every safeguard possible to eliminate or minimize the risk of injury which may lead to spinal injury.
Emergency service (lifeguards, law enforcement, fire suppression,and EMS) personnel must have the training and equipment to properly handle a suspected spinal injury in the aquatic environment. All aquatic facilities and emergency service agencies charged with the responsibility to provide emergency service in an aquatic environment must be equipped with appropriate spinal immobilization devices and flotation equipment for the handling of suspected spinal cord injuries in deep and shallow water.
Emergency service agencies and personnel can play a crucial role in the education of the public in the prevention of spinal cord injuries. This role can also be expanded to include the education of those persons (i.e., lifeguards) responsible for providing emergency care to suspected spinal cord injured persons resulting from activities in the aquatic environment.
References
1. Survey completed by the Research Triangle (NC) Institute for the National Institute of Neurological and Communicative Disorders and Stroke. JAMA, March 27,1981, Vol. 245 No. 12.
2. Summary of injury data of pools and spas, May 7,1985.